Journal of Diabetes Science and Technology, Vol. 7, Issue 1 Jan. 2013.
El-Gayar, Timsina and Nawar.
ABSTRACT
Background: Advancements in smartphone technology coupled with the proliferation of data connectivity has resulted in increased interest and unprecedented growth in mobile applications for diabetes self-management. The objective of this article is to determine, in a systematic review, whether diabetes applications have been helping patients with type 1 or type 2 diabetes self-manage their condition and to identify issues necessary for large-scale adoption of such interventions. Methods: The review covers commercial applications available on the Apple App Store (as a representative of commercially available applications) and articles published in relevant databases covering a period fromJanuary 1995 to August 2012. The review included all applications supporting any diabetes self-management task where the patient is the primary actor. Results: Available applications support self-management tasks such as physical exercise, insulin dosage or medication, blood glucose testing, and diet. Other support tasks considered include decision support, notification/alert, tagging of input data, and integration with social media. The review points to the potential for mobile applications to have a positive impact on diabetes self-management. Analysis indicates that application usage is associated with improved attitudes favorable to diabetes self-management. Limitations of the applications include lack of personalized feedback; usability issues, particularly the ease of data entry; and integration with patients and electronic health records. Conclusions: Research into the adoption and use of user-centered and sociotechnical design principles is needed to improve usability, perceived usefulness, and, ultimately, adoption of the technology. Proliferation and efficacy of interventions involving mobile applications will benefit from a holistic approach that takes into account patients’ expectations and providers’ needs.
J Diabetes Sci Technol 2013;7(1):247–262
rob halkes's insight:
There is good perspective to mobile health (ehealth) applications to self management in diabetes. However, as this research review suggests: we need to know more about use and socio technological influences. As I repeat myself: ehealth mhealth is NOT about technology: it is about implementation. Let's go for that!
After I published my white paper, The Guide to the Future of Medicine, the feedback was amazing and I had several really interesting (sometimes mind-blowing) discussions. One of these resulted in the idea of collecting those movies that predict, picture and demonstrate the future of medicine. Feel free to add your choices! Enjoy!.:
Elysium (2013)
Gattaca (1197)
Blade Runner (1982)
Brazil (1985)
Cloud Atlas (2012)
A.I. Artificial Intelligence (2001)
Eternal Sunshine of the Spotless Mind (2004)
Forbidden Planet (1956)
Inception (2010)
Prometheus (2012)
Robot & Franl (2012)
The fifth Element (1997)
rob halkes's insight:
Looking for visuals about the future of health, here they are ;-)
Clinical psychologists believe mobile technology applications geared to mental healthcare treatment have potential to improve patient care and practice management, based on a recent national survey conducted by market research firm Sigma Research. According to industry experts, the new research signals a readiness among mental healthcare professionals to adopt new mobile technologies that can bridge data gaps to improve therapy practice.
According to a survey of thousands of patients in Germany, Singapore, and the United Kingdom, the adoption of digital healthcare services remains low because existing services are either low quality or not meeting patients’ needs. The survey, conducted by consulting firm McKinsey, included responses from at least 1,000 patients in the three countries.
“Many healthcare executives believe that, due to the sensitive nature of medical care, patients don’t want to use digital services except in a few specific situations; decision makers often cite data that point to relatively low usage of digital healthcare services,” McKinsey analysts Stefan Biesdorf and Florian Niedermann wrote in a recent blog post. “In fact, the results of our survey reveal something quite different. The reason patients are slow to adopt digital healthcare is primarily because existing services don’t meet their needs or because they are of poor quality.”
McKinsey found that more than 75 percent of respondents would like to use some kind of digital health service. Many are interested in “mundane” offerings, the firm wrote.
rob halkes's insight:
Great Survey results, aligning with what experts already thought. Results generated by Germany, Singapore and the UK, but believed to be representative of patients in these advanced markets.
What is good medical engagement? In those organisations where it exists, how has good medical engagement been created and sustained? These questions are at the heart of this report, which builds on earlier work from The King’s Fund on medical leadership.
This report is based on case studies of four NHS trusts with acknowledged high levels of medical engagement. It aims to help other organisations that are seeking to create cultures in which doctors want to engage more in the management, leadership and improvement of services. Based on interviews with a range of executives, senior and junior doctors, the report presents key features of each of the four trusts. Its final analytical section highlights common themes and includes a checklist to allow organisations and individuals to assess how far medical engagement is being sought and developed.
Key Findings
Medical engagement needs to be part of an overall organisational approach, from board to ward, and needs time to evolve. It is a journey that requires doctors to be motivated and to assume greater engagement with and responsibility for improving the quality of patient care in partnership with clinical and non-clinical colleagues and with input from patients.
The four trusts studied have all enjoyed long-term stable leadership, creating a firm foundation for cultural change. Senior leaders have shown total commitment to medical engagement and leadership.
All four trusts have clear strategies based on quality running throughout the organisations. The distinguishing feature is that these strategies form a way of working for the organisation – they are not isolated programmes.
Each trust has embraced a strong medical leadership structure with doctors in leadership roles at divisional and departmental levels, supported by managers. Despite making great progress, none claims to have a completely embedded medical engagement culture.
Each trust puts considerable effort and resources into selecting senior staff including consultants, and none takes the stance that clinical expertise is sufficient.
Well-developed appraisal and revalidation processes exist in all four trusts. Talent management and leadership development are taken seriously, through education and training, and learning from other organisations.
Policy into practice implications
Medical engagement should be an integral part of the culture of all health care organisations and should be a priority for NHS boards and leaders.
It requires investment in development and training and also in governance arrangements to support the culture.
rob halkes's insight:
Must read to be inspired!
Report of case studies about developing "medical engagement." Although the term hasn't been defined precisely in the report it denotes its meaning at two points. It is stated that medical engagement is intended to lead to "...enhanced clinical and organisational outcomes, and to real benefits for patients and staff.."(p.39). Also, it is said in the conclusions, that a "..sustained and collective vision" .. will enable to create an "..organisational culture where all staff, particularly doctors, are motivated to share in delivering the highest quality of care." (p.41)
In summary, what is needed to bring about this fundamental change, is, in my words:
- an overall and integrated program, led by explicit starting points that may act as a guiding philosophy,
- a collective leadership that endorses and leads the change,
- explicit selection of doctors and staff, with the needed attitude and intentions, also a program of development, training and learning that initiates and continues inspiration to the right development, and
- enough time to make it work and allows for genuine change.
So, in retrospect, the report tells us that change and development is hard work like any implementation of innovation and development. The distinction here, in the report, is the concrete case findings and examples of how it was brought about. That makes it very worthwhile to read it.
However, some comment is in order: patients' benefits are only indicated but mostly absent from the report. It is all about the staff and doctors' activities directed to "medical engagement" - a strange term for a self evident responsibility to a medical institute. But if the terms helps to motivate, that is fine with me, but in my personal reflection, in these cases, it has little to do with patient engagement.
Add to the project a working method with patients, in a co-creative way and patient benefit will readily arise! See here for further information about co-creation in care.
Diseases of the adrenal gland have long been difficult to diagnose. But now, researchers have found an affordable and easy way to diagnose and monitor endocrine diseases of the adrenal gland by using saliva and a smartphone.
Researchers at Intermountain Medical Center in Murray, Utah, have developed new smartphone technology to help screen patients for a number of adrenal gland diseases, including Cushing's syndrome. The new tool also helps to identify adrenal insufficiency, monitor cortisol replacement and assess physiologic changes in adrenal function.
Adrenal diseases are commonly overlooked because measuring cortisol, the so-called "stress hormone" that is released by the adrenal glands as part of the fight-or-flight mechanism, is costly and complicated, especially for those with limited resources, say researchers.
"When cortisol levels are overlooked too many people suffer and die because of excess or insufficient cortisol," said Joel Ehrenkranz, MD, director of diabetes and endocrinology at Intermountain Medical Center, and lead researcher of the project.
To help solve this problem, researchers developed a simple saliva test that uses a smartphone and an attached device that inexpensively feeds the results of a saliva test into the smart phone. An app then quantifies and interprets the results of a salivary cortisol assay and gives results in five minutes at the point of care.
"The cortisol assay is similar in design to a home pregnancy test and urine sample drug tests," says Dr. Ehrenkranz. "It's like having an endocrine specialist in your phone."
[...]
The new technology will especially help diabetic patients.
For diabetics, controlling stress levels is key to controlling cortisol levels, which helps prevent and control the disease. Stress increases the levels of cortisol in their body, and elevations in cortisol impair the body's ability to metabolize glucose. This increases blood glucose levels. High cortisol levels also affect the body's ability to fight infections, lose weight and recovery from injury.
"What this means is when blood cortisol levels are too high, insulin will not lower blood sugar," said Dr. Ehrenkranz. "Elevations in cortisol decrease the effectiveness of insulin and other drugs used in the treatment of diabetes. Having the ability to easily and inexpensively measure cortisol levels is important in managing diabetes."
See also http://mobihealthnews.com/34753/intermountain-researchers-develop-smartphone-based-lab-test-for-stress/
rob halkes's insight:
Great example of Intermountain Health development of Mobile Med Tech - a first step into further development of ehealth eco systems for diabetes and other chronic diseases needing "..to identify adrenal insufficiency, monitor cortisol replacement and assess physiologic changes in adrenal function"
This development however will take some next steps into adopting the right processes and actions to create functional interaction with patients. I would say: go on! ;-)
Use of social networking services (SNS) is on the rise. While many users sign in for personal purposes, it is not uncommon for professionals to connect over SNSs with clients, students, and patients.
Methods
The present study used an experimental approach to examine how medical doctors’ SNS profiles impacted potential patients’ impressions of professionalism. Participants (N=250 students) were randomly assigned to view one of six Facebook profiles. Profiles were populated with 1) solely professional material, 2) personal material that was strictly healthy, or 3) personal material that included unhealthy behavior. Profiles portrayed a male or female physician resulting in a total of six experimental conditions. Medical professionalism was measured with the First Impressions of Medical Professionalism (FIMP) scale, specifically developed for this study.
Results
There was a large and statistically significant main effect for profile type, F(2, 250)=54.77, p<0.001, η2p=0.31 Post hoc tests indicated that personal profiles that contained healthy behavior were rated as most professional followed by profiles with strictly professional content. Personal unhealthy profiles were rated as least professional. Additionally, female profiles consistently received higher professionalism ratings across all three profile types [F(1, 250)=5.04, p=0.026, η2p=0.02].
Conclusion
Our results suggest that a physician's SNS profile affects a patient's perception of that physician's medical professionalism. A personal, healthy profile may augment a patient's perception of that physician's character virtues if the profile content upholds the decorum of the medical field.
Keywords: professionalism, Facebook, professionalism scale, social networking
rob halkes's insight:
Two statements come to mind when reading this report:
1) Doctors/Physicians: when you intend to be active on social media, be sure first to adopt a healthy life style yourself..;
2) Patients: it proves you right in the way you interpret your doctors' professionalism - let it guide you in your preferences
Very interesting and must read piece on how doctors present themselves on social media!
Pins about Customer "hand-picked" by Pinner Rob Halkes | See more about customer experience, infographic and marketing.
Health care development is in the business of creating more patient - professional interaction in health care, improving interaction, communication and understanding. In preparing my consultancy work, e.g. to help health care professionals with co-creating care, I came across these pins. Maybe you like them.For your information see here: http://www.healthbusinessconsult.com/co-creation-in-health-care/
rob halkes's insight:
Pins with regard to putting "customers" first: how to, like mapping the customer journey and/or customer experience. Imagine when health care professionals would work like this..;-)
What’s next on the horizon for doctors and patients? Medical experts predict the biggest changes likely to occur in primary care over the next decade. [...]
- Doctors will rely on Wearbale tech for Real-time Insights..
[...]
- Waiting Rooms will be phased out ..
[...]
- Up to 35 Percent of Visits Will Happen Virtually—Or Not at All
[...]
- Patients Will Increasingly Control Their Medical Charts
[...]
The key for success, Burgert says, is for physicians to push through the learning curve and anxiety associated with many new technologies and be open to the changes that lie ahead. She explains: “Physicians who maintain their willingness to listen and learn, despite the common anxiety of not knowing everything in uncharted territory, will be better positioned in the future.”..
rob halkes's insight:
In the spirit of the trends, this oversight confirms them. See here and more specifically about what should be the trends here.
Interesting ans inspiring however are the data mentioned in the referred studies, from Wolters Kluwer and from Software Advice.
And surely: health care professionals need to "push through the learning curve.." - Great statement ;-)
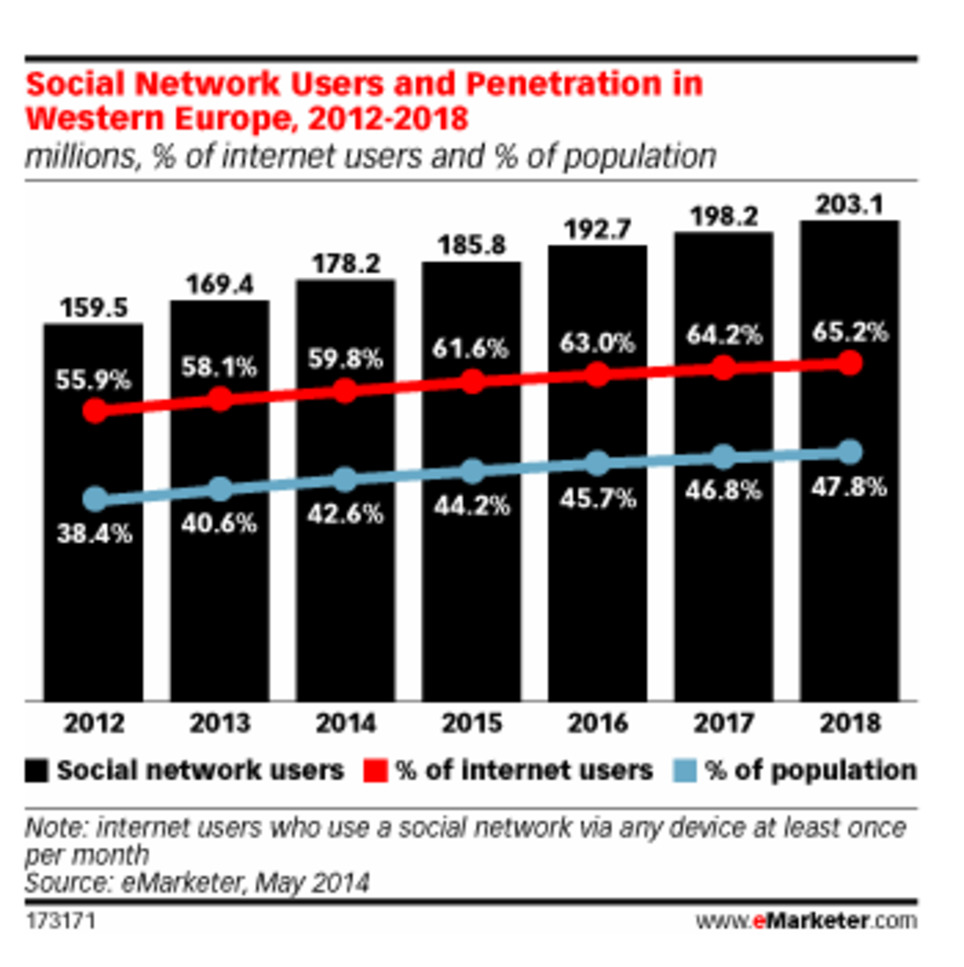
Advertisers in Western Europe will spend $2.54 billion this year on social network ads to reach the region's 178.2 million social users, according to a new eMarketer report. While privacy concerns remain an issue, Western Europe's social networkers often put them aside for personalized experiences.
rob halkes's insight:
Yes we knew about this trend, but THE question remains whether this goes the same for all other kind of services AND for health services? I don't think so if i take myself as representative example, but one never knows. I 'll be happy with anyone knowing about research with this distinction?
Experience co-creation in health care is an effective method to innovate value to patients in a personalized way, in collaboration with all relevant stakeholders. It is intended to benefit patients in coping with their health conditions and to arrive at a satisfying state of quality of life, given their specific personal health conditions.
Working together is conditional to health care. But "Co-Creation" and "Experience Co-Creation" are not like “working together” in a traditional way. The concept of the method of co-creation is rather based on acknowledging the difficulties in health care to work together. “Experience co-creation in care” enables personalization of health care tailored to the patient conditions and preferences. It drives the effectiveness of the total process: efficacy of medical interventions, therapy, rehabilitation and lifestyle.
rob halkes's insight:
I just wanted to create a quick overview of what Co-creation in Care looks like.
The Dutch national eHealth monitor was conducted by Nictiz and NIVEL. The survey monitors the availability and use of eHealth applications by healthcare users and healthcare providers.
See the summary through this link. You kay also download here ..
rob halkes's insight:
The Netherlands score very well on progress in eHealth. But the conclusion of the monitor is: there's is still a lot to be done ...
Recognizing that licensing and regulation has not kept pace with the growth of telemedicine applications, a new report offers five recommendations for the successful adoption of telehealth.
The recommendations, made by the Information Technology and Innovation Foundation, a District of Columbia-based think tank, include:
Great blog and great report: concluding about the necessary steps to enable the development and implementation if ehealth over multistakeholders, health care providers and industry.
Not all have been copied here. so do read the report and the blog..!
It’s been 10 years this month since Fred Lee published his book “If Disney Ran Your Hospital: 9 1/2 Things You Would Do Differently.” The book offers hospital administrators and service line directors key insights for transforming their “services” to “experiences,” including:
Generating loyalty by doing memorable things that patients don’t expect
Being alert on people’s needs and taking initiative, before they ask for it
Shifting from “our services” to the guest’s story
Over the past year, the Disney team – masters at consumer engagement – has transformed their entire experience with the addition of their MyMagic+ program. Hospitals can take this opportunity to learn from Disney’s leading-edge strategies about where experiences are going next:
The Move To Digital ...
Online Planning Ahead from Home ...
Personalization ...
Collaboration ...
At first glance, these may all look only like guest benefits. However, every interaction produces a bit of valuable guest-generated data, and Disney uses the data to learn more about what works and what needs improvement in their entire operation. They can better understand patterns of guest behavior and desires. They can quickly uncover dissatisfiers. They will have insights into which rides and restaurants are pulling their weight and which are not. Plus, they can better tailor each guest’s offer for their next visit based on past behavior. This kind of real-time data goes way beyond satisfaction surveys. Its wired back into the process to create a fast loop for continuous improvement.
Beyond data advantages, when guests take the time to plan in advance, it produces operational efficiencies for improved capacity and revenue growth. Disney recently stated the technology investment is beginning to pay off in: increased park capacity (more volume), visitors spending more time on property (more money), and a better experience (more loyalty). A great example demonstrating that being centered on the guest and their experience results in benefits for the provider.
Today, digital patient engagement technologies offer the same vision for healthcare: A personalized end-to-end patient-centered experience with at least one “memorable moment.” Patients preparing for surgery or working on treatment care plans from home, collaborating with friends and family online. True visibility for administration on what’s working and what’s not in their programs. Sound like a place “Where Dreams Come True”?
Focusing on what the patient wants, and needs to cope with his or her conditions and therapy is a great principle to follow. Patient advocates, epatients, interviews, analysing the "patient journey" through your health care, gathering data about his or her activities/behaviour - all will open your window to insights about them. Take the effort!
Even hospitals with the sturdiest reputations are having a hard time extending their digital presence and offering expertise beyond the confines of a brick-and-mortar hospital, according to a new report from Evolve Digital Labs.
This first-of-its-kind report, "The Digital Health of Today's Best Hospitals," evaluates the online presence and patient use of digital assets or websites from some of the top hospitals in the country, as identified by U.S. News & World Report. Hospitals and health systems analyzed include Massachusetts General Hospital in Boston, UPMC in Pittsburgh, Hospital of the University of Pennsylvania in Philadelphia and University of Texas MD Anderson Cancer Center in Houston, among many others.
Here are 10 key findings and points of analyses from the report.
1. Even top brands struggle. Derek Mabie, president of Evolve, said the most remarkable finding from the report is how top healthcare brands struggle to expand their presence on digital platforms or meet consumers' expectations for mobile access ...
2. Key findings. The study analyzed 57 hospitals from January 2013-January 2014. ..
The analysis found: • 49 percent of hospitals lacked a mobile patient website • 67 percent failed to offer online rehabilitation and aftercare information • Only 1 in 5 had online pre-registration to reduce patient wait time • Nearly 1 in 3 failed to facilitate online bill pay • At least 18 percent had onsite errors that hindered the patient experience • Nearly 1 out of 2 hospitals did not support post-prescription refill requests online
3. Barriers systems face. Mr. Mabie recognizes some barriers that may hold hospitals or health systems back in their digital efforts. "Clinical oversight of content is probably a barrier.... 4. The need for digital governance. Mr. Mabie also says the report highlights the need for digital governance across healthcare organizations to fill the communication gap between patients, clinicians, health IT experts, marketing and communication teams...
5. The top 10 patient-centric hospital websites, according to the report, are:
• Mayo Clinic (Rochester, Minn.) • Cleveland Clinic • University of Texas MD Anderson Cancer Center (Houston) • Massachusetts General Hospital (Boston) • UPMC (Pittsburgh) • Duke Medicine (Durham, N.C.) • Thomas Jefferson University Hospital (Philadelphia) • Massachusetts Eye and Ear (Boston) • The Mount Sinai Medical Center (New York City) • Florida Hospital (Orlando) 6. Determining patient-friendliness. To determine whether a website was patient-friendly, the study looked for websites that offered options to complete medical forms before appointments, make appointments, request refills, pay medical bills, view medical records and/or tests and view discharge and rehabilitation information. ..
7. Google results and brand reach. Search result rankings are one component of a hospital's brand reach score. ...
8. Mayo Clinic did best in search results. ..
9. There is a distinction between patient- and brand-centric website content, and some hospital websites can cross this line without even knowing it ...
10. The link between digital presence and spending. Hospitals' subpar digital presence isn't so much the result of hospitals' crunched finances, but more about leaders thinking money spent on website development is not worth it. "I'd say if they truly understand ROI and their ability to capture metrics, most would invest at much greater level," says Mr. Mabie. "It's the most scalable way to reach people.
rob halkes's insight:
Indeed I wondered a lot times why a hospitals' website seems to be so unuser friendly, nor give adequate lenience t finding what you want. May these 10 might be at the bottom of that. A good guide for hospital staff to review.
On February 18th we gathered a panel from across three continents to discuss e-patient and physician relations in our latest Doctors 2.0 & You Google hangout.
Moderated by ePatient and health blogger, Marie Ennis-O’Connor, the panel which included Denise Silber (founder of Doctors 2.0), Jamie Tripp Utitus (MS survivor and health blogger) and Renza Sciblia (diabetes consumer and health blogger) discussed the ways in which new technologies are contributing to the patient/physician relationship. The following is a summary of the discussion, which can be viewed in its entirety via the video below.
Relationships in medicine are as important now as they were in the past. The difference is that today’s technology allows physicians and patients to communicate on a different level. The panel listed some of the new technologies that are changing the dynamic between the patient and the physician, and how the balance of power has shifted.This led to a discussion on how some doctors view the empowered, digitally savvy patient as a challenge to their authority and expertise. Jamie suggests leading physicians gently towards a discussion on health technology, while Renza sees this as an opportunity to broaden the relationship between doctor and patient, fostering more openness and honesty in the relationship. She suggests that patients interview their doctors in advance to find the level of collaboration they are happy with.
Speaking to the numbers of doctors who embrace new technologies, Denise suggests that this is a multi-factorial problem, encompassing people skills and financial remuneration. Michael Weiss, listening online to the discussion, asked the panel for their thoughts on the future of medicine being the convergence of ehealth, mobile health and social media. The panel are all in agreement that this is the future of medicine, and spent some time on the important role that social media has to play in supporting and educating patients. Blogs and Twitter chats are great vehicles for healthcare professionals to learn about the lived experience of a condition.
The discussion ended with each panellist offering one piece of advice to physicians to help them prepare for a future where patients are empowered by new technologies. Renza’s advice is to just step in there and offers the reassurance that the majority of patient sites online are very well moderated and provide accurate information. This is not about replacing the doctor/patient relationship, but augmenting it. Jamie refers to Dr. Charles Safran’s quote that patients are the most underutilized resource in healthcare, followed by Denise quoting that the patient is the first member of the medical team. The discussion ends with Jamie’s call to patients to join the healthcare conversations online – to find answers and support and Renza emphasizing the peer-to-peersupport and power of community that can be accessed online.
rob halkes's insight:
Everything in ehealth and telehealth has to do with improving data sharing, interaction and communication between the patient and his/her professional supporters. This is an inspring dicussion to this aim!
Video maps growth in doctors, nurses and healthcare professionals using Twitter since its launch in 2006 to 2014. Data sourced using Creation Pinpoint, the world's largest reserach too for learning from heathcare professionas in public media...
rob halkes's insight:
Said a lot about Doctors on Twitter. Now have a look at its growth! It is inspiring! Thx CreationHealthcare.
Social Media: A Review and Tutorial of Applications in Medicine and Health Care
Background: Social media are dynamic and interactive computer-mediated communication tools that have high penetration rates in the general population in high-income and middle-income countries. However, in medicine and health care, a large number of stakeholders (eg, clinicians, administrators, professional colleges, academic institutions, ministries of health, among others) are unaware of social media’s relevance, potential applications in their day-to-day activities, as well as the inherent risks and how these may be attenuated and mitigated. Objective: We conducted a narrative review with the aim to present case studies that illustrate how, where, and why social media are being used in the medical and health care sectors. Methods: Using a critical-interpretivist framework, we used qualitative methods to synthesize the impact and illustrate, explain, and provide contextual knowledge of the applications and potential implementations of social media in medicine and health care. Both traditional (eg, peer-reviewed) and nontraditional (eg, policies, case studies, and social media content) sources were used, in addition to an environmental scan (using Google and Bing Web searches) of resources. Results: We reviewed, evaluated, and synthesized 76 articles, 44 websites, and 11 policies/reports. Results and case studies are presented according to 10 different categories of social media: (1) blogs (eg, WordPress), (2) microblogs (eg, Twitter), (3) social networking sites (eg, Facebook), (4) professional networking sites (eg, LinkedIn, Sermo), (5) thematic networking sites (eg, 23andMe), (6) wikis (eg, Wikipedia), (7) mashups (eg, HealthMap), (8) collaborative filtering sites (eg, Digg), (9) media sharing sites (eg, YouTube, Slideshare), and others (eg, SecondLife). Four recommendations are provided and explained for stakeholders wishing to engage with social media while attenuating risk: (1) maintain professionalism at all times, (2) be authentic, have fun, and do not be afraid, (3) ask for help, and (4) focus, grab attention, and engage. Conclusions: The role of social media in the medical and health care sectors is far reaching, and many questions in terms of governance, ethics, professionalism, privacy, confidentiality, and information quality remain unanswered. By following the guidelines presented, professionals have a starting point to engage with social media in a safe and ethical manner. Future research will be required to understand the synergies between social media and evidence-based practice, as well as develop institutional policies that benefit patients, clinicians, public health practitioners, and industry alike.
rob halkes's insight:
Social Media is going to play a significant rol in health care. It may have a farreachiung implication indeed. But we still have to see and observe how that is going to happen. What we however ought to do, is to see how we change health care to better outcomes and fewer costs, to prevent that the "disruption of care" will have consequences we don't want.
For hundreds of years, the physician-patient relationship has seen the physician as the authoritative, sometimes dictatorial, healer — the unquestioned expert on care, protocols and medical regimens. The patient assumed the role of a passive receiver of information, taking orders and instruction from the doctor.
Today, there is a movement afoot — one that is welcomed by me and many of my colleagues. It’s a change that I hope will become the norm when it comes to the physician-patient relationship. It’s all about partnerships between patient and provider.
Participatory medicine, as noted by the Society for Participatory Medicine (S4PM), is “a movement in which networked patients shift from being mere passengers to responsible drivers of their health and in which providers encourage and value them as full partners.”
The society further states, “Participatory medicine is a model of cooperative health care that seeks to achieve active involvement by patients, professionals, caregivers, and others across the continuum of care on all issues related to an individual's health.”
I encourage my colleagues and medical professionals across our region to embrace the participatory medicine movement.
read on!
rob halkes's insight:
Participatory medicine - a "must" in the transformation of care. Marc Katz MD writes a must read introduction to his colleagues about the movement. Why don't you have a look by yourself, at least if you haven't heard of participatory medicine before!
The consent process for opting out of care.data should be clear and transparent, and patients should be the first to have access, says Mohammad Al-Ubaydli
The case the government makes for care.data, that allowing medical researchers access to patient data will result in new cures, is a hard one to oppose. If the case were so simple then most people, including me, would welcome it.
The question that the care.data effort brings to light is a simple one – why has the NHS moved so quickly to provide patient medical records to third parties and so slowly to provide data to the patient themselves? For me, this is entirely the wrong way round.
The consent process for opting out of care.data is neither clear nor transparent. The questions page states that the record will not contain information that can identify a patient – and it's true that NHS number, postcode, full name etc will be removed. However, it's also true that each patient's record will be linked to a "meaningless pseudonym that bears no relationship to their 'real world' identity".
The information being shared by care.data is substantial. They exclude sexual health data, such as HIV diagnosis or abortions – but they include mental health data. They exclude written notes – but they include actual diagnoses, medications and laboratory results.
In addition, the records will be shared with third parties a patient might not want to have their data. HSCIC public assurance director Dr Mark Davies has already said that, in the eyes of the law, the government can't distinguish between a request by an insurance company and a medical researcher to access the database. For them, it makes no difference. But it makes a difference to the patient, who could, would and should distinguish. Indeed, at the moment the patient isn't even allowed to see data in their own record that third parties will have access to.
Government representatives repeat in interviews that they need to open a debate on care.data – so let's have the debate now while plans have come to a temporary halt. We know from other countries that a proper discussion on government-controlled data leads to different outcomes. ...
The government says that care.data can bring huge benefits. If so, it needs to prove what these benefits are and start by giving the patients themselves data about their own bodies.
National health record systems should be furthered by giving the patient first access to their information. First, because patients are best suited for checking those data for which they are the only right source for checking it, e.g. their medications: think about actual use. They are the sources for checking "actuality": what is actually being "used", "validity": is the right information given - does it represent what is "on" and what not, and "reliability" is everything in the right terms and details (doses for instance). That is the instrumental use of patient access, besides the principle use of it: patients ought to have insights in their formal data and functional use of it: by sharing same information and data the protagonists in care for patient's health can do a better job together for better health outcomes. ..
Australian patient don't have access to our own health data, diagnoses, medications, lab test results; surely that is a fundamental right! The PCEHR is the dream, not the reality of delivering this.
This week on March 5, I'm delighted to have long-standing #hcsmca member and co-founder of #hcldr chat Colin Hung lead a discussion on patient engagement. I'll let Colin explain.
Last week I had the privilege of attending the 2014 annual HIMSS conference in Orlando Florida. Every year, I’m amazed and inspired by all the innovative people, products and projects that are presented or on display. This year was no exception.
One of the trending topics this year at HIMSS14 was patient engagement. For me this was particularly exciting. For years many of us on social media, especially those of us who participate on #hcsmca and other chats, have been advocating for more patient involvement in healthcare. Together we have helped to push the industry towards true patient-centred care and truly engaged patients.
In 2012 Leonard Kish (@leonardkish), a well-respected Healthcare IT consultant, wrote an amazing blog post, The Blockbuster Drug of the Century: An Engaged Patient, that showed how patient engagement could be the “blockbuster drug” of the year. In his post, Kish provides very compelling statistics:
19.74% reduction in hospital admissions
25.31% reduction in bed days of care
86% patient satisfaction
$1,600 average cost per patient per year, compared to $13,121 for primary care and $77,745 for nursing home care
20% to 57% reduction in the need to be treated for the chronic diseases studied, including diabetes, COPD, heart failure, PTSD, and depression
As I was touring the HIMSS14 exhibit hall, I was reminded constantly of Kish’s post. Almost every vendor had some form of patient engagement technology. ..
I began to wonder about the definition of patient engagement and whether or not it would be worthwhile for the healthcare IT industry to have a common definition. It’s my belief that armed without a standardized definition or widely accepted market norm, we’ll continue to see poorly conceived engagement technologies that do little more than throw patient data onto a screen...Pat Rich (@cmaer) wrote an excellent Day 1 summary of #HIMSS14, The patient has no clothes, where he commented about how challenging patient engagement will be to operationalize:
“…while the majority of patients will discover errors in their own records when they evaluate them, there are few mechanisms or resources in place for doctors’ offices to correct those records … and many physicians are unprepared for the impact truly engaged patients will have on their workflow.”
I believe that almost everyone would agree that becoming more involved and engaged in your own health and healthcare is a good thing. But what does being an engaged patient really mean? Is it possible to come up with a single definition that we can all agree to? ...
rob halkes's insight:
Great observations. Indeed large volumes of interests.. Interests in both meanings of curiosity and of weight (in the sense of self-interest) are high in this case. After a history of telling patients what to do (see for instance http://sco.lt/7DGqp7 ), it will be no wonder that we really do want change to happen, but that is tricky. As Pat suggests: let’s do some research and in any case let’s write evaluations of any trial or pilot we undertake. It will not be easy surely. That’s why I was thinking in building efforts to cooperation among protagonists. I gave a description of it here: http://bit.ly/1icTOvZ . I’m curious of what you think of it. By the way co-creation and co-creation of experience is an excellent method to process coordination in this.
To get content containing either thought or leadership enter:
To get content containing both thought and leadership enter:
To get content containing the expression thought leadership enter:
You can enter several keywords and you can refine them whenever you want. Our suggestion engine uses more signals but entering a few keywords here will rapidly give you great content to curate.



 Your new post is loading...
Your new post is loading...































{kind=link}
There is good perspective to mobile health (ehealth) applications to self management in diabetes. However, as this research review suggests: we need to know more about use and socio technological influences. As I repeat myself: ehealth mhealth is NOT about technology: it is about implementation. Let's go for that!